

In 2022, C-TAC expanded our relationships on the Hill, deepened our engagement with state leaders, and continued our dialogue with the Administration through our regulatory and administrative advocacy. This year our focus remains on creating a continuum of care for patients and their families from diagnosis through to the end of life, working with innovative care models such as: Home-Based Primary Care, Palliative Care, PACE, and Hospice. In the past few months of 2023 there have been a number of opportunities – highlighted below – to advance C-TAC’s agenda at the federal level and, increasingly, with states.
1) Payment Demonstrations – Center for Medicare and Medicaid Innovation (CMMI)
CMMI continues its commitment to our population. In a recent publication CMMI cites challenges with enrollment along with program design and ROI in expanding demonstrations for those with serious illness.
- CMMI recently looked at data from recent demonstrations that showed:
- Beneficiaries and caregivers reported high satisfaction with palliative support.
- Participating sites struggled to reach and enroll their target populations due in part to low referrals from primary care providers and specialists.
- Sutter Health’s palliative care program – Advanced Illness Management — showed significant decreases in Medicare spending.
- C-TAC Next Steps with CMMI
- We will continue to work with the Innovation Center to integrate palliative care into the new Accountable Care Organization Realizing Equity, Access, and Community Health (ACO REACH) model, Medicare Advantage Value-Based Insurance Design (VBID) model and Enhancing Oncology Model (EOM).
- Our case is that a comprehensive approach to palliative care, including access to interdisciplinary teams, home visits, and shared decision-making, could improve care, appropriately adapted to the target population and setting.
2) Advocating for the Consumer in Hospice Reform
The time has come for hospice reform and “modernization.” We need to bring the latest knowledge, methods, and innovations to the hospice movement to improve the quality of care and integrity of the program and expand its benefits to more individuals with serious illness.
There are two approaches and discussions underway in the nation’s capital to accomplish this, one concerning the integrity of the industry amid concerns of fraud, waste, and abuse. First, four major hospice providers organizations have put forth a set of 34 Hospice Program Integrity Ideas to the Centers for Medicare & Medicaid Services (CMS) and other policymakers to address problems and improve program integrity. C-TAC supports the work of the provider organizations. To further advance improvement, C-TAC is focusing on the value of consumer information, quality assurance, and consumer rights in these discussions.
The second approach targets the long-term future of the hospice benefit and how it should be modified to improve the lives of more individuals with serious illness and their family caregivers. C-TAC has been invited to the table to help guide the process of modernizing the hospice benefit on behalf of consumers. C-TAC is collaborating with the National Partnership for Healthcare and Hospice Innovation (NPHI) and Hill staff to explore ways to strengthen and expand the benefit and provide better coverage for palliative care services and community-based supports for individuals with serious illness “up-stream” from current hospice eligibility.
We have been working closely with Rep. Blumenauer (D-OR, 3rd), who is a leader on this and other serious illness issues on the House Ways and Means Committee, as well as with his personal staff and committee staff. On the senate side, we have a champion in Senator Mark Warner (D-VA) on the Finance Committee, who in addition to sponsoring the advance care planning bill that C-TAC has championed, is also committed to strengthening the Medicare hospice benefit and expanding palliative care.
Hospice is an amazing Medicare success story that provides a range of services that are so important to individuals and families dealing with serious illness. C-TAC supports hospice modernization to improve the quality of care for those with serious illness, including:
- Reform of the limitation of the six-month prognosis rule to support this successful team-based approach to care earlier in the course of serious illness;
- Allowing concurrent care coverage; and
- Covering upstream palliative care services and supports and services.
We also believe that an early comprehensive assessment is key to enabling the right care at the right time, especially for palliative and hospice care. A comprehensive assessment should assess each person’s physical, social, psychological, and spiritual needs and the needs of the family caregiver(s) on an ongoing basis. This assessment and subsequent care coordination is essential to ensuring that the necessary resources are made available to the individual based on their care preferences and that the most efficient and often also the most-cost effective service delivery is used. We will strive to make this a part of the discussions on program improvements. The aging network (e.g., Area Agencies on Aging) and community-based faith-based organizations are valuable partners in this work.
As a diverse coalition, C-TAC’s strength lies in the fact that we all agree on a core set of principles that emphasize a person-centered, consumer-oriented focus on the needs of individuals and families throughout a serious illness. We see hospice modernization as an opportunity to work toward the goal of health equity, as well, since we advocate for particular attention to individuals living with serious illness who are underserved and under-resourced.
3) Advance Care Planning – A Key Intervention
In January, the Office of the Inspector General (OIG) released a report on the usage of the Advance Care Planning CPT Codes.
- Medicare providers were paid approximately $42.3 million for Advance Care Planning (ACP) services that did not comply with Federal requirements.
- These payments occurred because the providers did not understand the Federal requirements for billing ACP services.
- OIG recommends that CMS educate providers on documentation and time requirements for ACP services to comply with Federal requirements and CMS has concurred with this recommendation. Note: we support this recommendation and had suggested it to OIG when we spoke with them earlier in 2022.
- In 2022, C-TAC worked with Rep. Ed Blumenauer (D-OR-3rd) and Sen. Mark Warner (D-VA) on the bipartisan bill “Improving Access to Advance Care Planning Act” (H.R.8840/S.4873). Sen. Susan Collins (R-ME) also co-sponsored the bill. The bills’ sponsors were unable to secure any of the provisions in the end of the year Consolidated Appropriations Act, 2023, but pledged to reintroduce the bill in the 118th
- For more information, see our blog post
4) Accelerating State Policy
In an effort to support our federal policy agenda, C-TAC is convening States committed to new models of care within their Medicaid programs to support people with serious illness and improve health equity.
- Hawaii is leading this effort and has already filed a state plan amendment with the Center for Medicaid and CHIP Services (CMCS) to create a community palliative care benefit, while other states have passed relevant state legislation directing inquiry into such benefits.
- We have asked CMCS to issue federal policy guidance on serious illness, which they haven’t done since 2011 (concurrent hospice care for children). This will help to prioritize key areas of state need and support our CMS policy champions in standardizing key aspects of serious illness care.
5) Recent Medicare Advantage Policy Developments affecting Serious Illness
Starting in 2024, more older adults will be enrolled in MA than in traditional Medicare. Given that, MA policies and oversight will be important to those living with serious illness. Opportunities we are pursuing include:
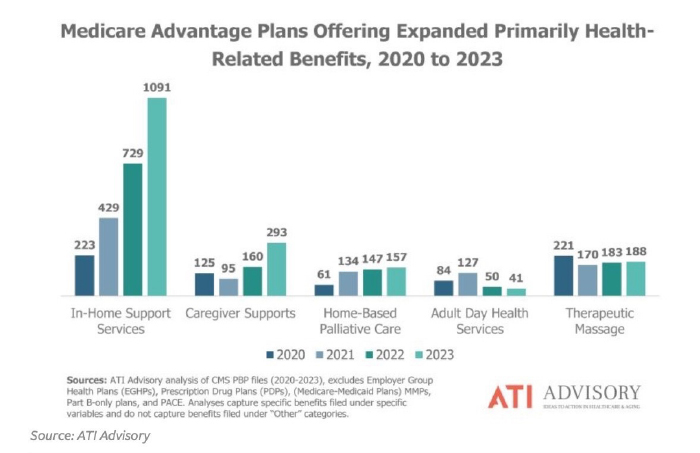
- Supplemental Benefits (SBs)– In 2019 CMS expanded possible SBs to include home-based palliative care, support for family caregivers of enrollees, or adult day care. In-home services are now very prevalent, see graph below, although the uptake of home-based palliative care programs has been slow with only 65 plans offering them in 2020, increasing to 157 plans in 2023:
- Hospice Carve-in through the MA VBID Model– The VBID model is a CMMI payment model that began in 2017 and has just been extended through 2029. It allows MAOs the flexibility to vary their benefits for enrollees with a limited set of clinical conditions using value-based approaches to service delivery; there is also the opportunity to offer enrollees additional services, including non-hospice palliative care for those not eligible for hospice care, transitional concurrent care through in-network providers to help ease enrollees’ transition to hospice, and SBs to provide additional coverage, items, services, or supplies to support enrollees in hospice.
- Special Needs Plans (SNPs) for People with Serious Illness– SNPs are an MA coordinated-care plan designed to provide targeted care to special needs individuals. SNP enrollment increased from 3.8 million in 2021 to 4.6 million in 2022, +20%, and most SNP participants live with serious illness.
- Equity Efforts– MA beneficiaries have lower incomes, are more likely to speak English as a second language, are more likely to rent their home, and are more reliant on public transit than those enrolled in traditional Medicare. Therefore, CMS is focused on tracking social determinants of health (SDOH) in MA plans. The proposed MA rule for 2024 includes required SDOH assessment along with a payment bonus opportunity. CMS proposed a health equity index (HEI) reward to further encourage MA plans to improve care for beneficiaries with certain social risk factors. This is an example of a new payment mechanism to promote health equity that may be expanded to other Medicare programs if it is effective.
6) Recent Executive Orders Supports Caregivers, In-Home Care
On April 18, the Biden-Harris Administration announced Executive Orders (more than 50) to address the needs of care workers, family caregivers, long-term care workers, veterans, kids/childcare, early educators, and issues of recruitment, retention, and training for direct care workers (compensation, job quality), and care accessibility. President Biden called for executive departments and agencies to do what they can within their authorities to address the supply of high-quality early care and education and long-term care and called on Congress to provide significant new federal investments to transform care in the U.S. and “give families in this country more breathing room when it comes to care.”
Opportunities for C-TAC within these Orders include:
- Dementia Care: Health and Human Services (HHS) is directed to consider testing a new dementia care model that will include support for respite care (short-term help to give a primary family caregiver a break) and make it easier for family caregivers to access Medicare beneficiary information and provide more support to family caregivers during the hospital discharge planning process. Palliative care will also be included in the model, we believe.
- Family Caregivers: Many of the Orders come right from the RAISE Family Caregiver strategies. They also call for rulemaking by the Veterans Administration (VA) on eligibility criteria for its family caregiver assistance program for caregivers of veterans with serious illness or injury from active duty.
- Home-Based Models and Supports for Veterans:
- The VA will consider adding 75 new interdisciplinary teams to its Home-Based Primary Care program.
- HHS is directed to consider issuing several regulations and guidance documents to improve the quality of home care jobs, including by leveraging Medicaid funding to ensure there are enough home care workers to provide care to seniors and people with disabilities enrolled in Medicaid, as well as build on the minimum staffing standards for nursing homes, and condition a portion of Medicare payments on how well a nursing home retains workers.
- The VA is directed to consider expanding its Veteran Directed Care program to all 172 VA Medical Centers by the end of Fiscal Year 2024. This program provides veterans with a budget to hire personal care assistance including from family members.


