
The Issue and Background
As the U.S. population ages, there is increasing recognition of the complex, intertwined needs of individuals living with serious illness and behavioral health conditions.
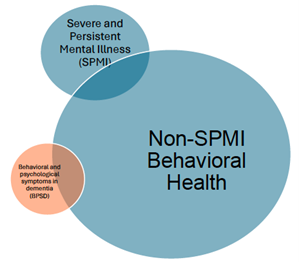
Behavioral health conditions affect a wide range of people with serious illness and may present in various forms. Many individuals may have experienced longstanding serious and persistent mental illness (SPMI) such as schizophrenia, bipolar disorder, or severe depression prior to developing a serious physical illness. Others may develop depression, anxiety, or substance use disorders as a result of the challenges and losses associated with living with serious illness. Still others, especially individuals with dementia, may experience behavioral and psychological symptoms that may resemble mental illness and complicate disease management and quality of life. These categories are not mutually exclusive and often overlap, creating complex care needs that cut across traditional medical and behavioral health boundaries.
Together, these overlapping populations represent millions of Americans:
- At least 13 million adults and 700,000 children live with serious illness in the United States
- Nearly 10 million older adults experience any mental illness, including 1.5 million who experience SPMI
- Prevalence of co-occurring mental and physical illness is hard to measure, but one study found that 60% of patients experiencing heart failure experienced depression and anxiety.
- An estimated are living with Alzheimer’s disease or other dementias, a number projected to nearly double by 2060. Approximately 90% of individuals with dementia will experience behavioral and psychological symptoms of dementia (BPSD)—such as agitation, depression, hallucinations, or sleep disturbances—during the course of their illness.
Many of these individuals fall through gaps in the health care system due to fragmented behavioral and medical services, workforce shortages, and payment misalignment.
Clinical and System Gaps
Existing models of care often do not sufficiently acknowledge the complex interaction of physical and behavioral health needs. Depending on where individuals seek care, the treatment models can vary widely:
| A cancer patient with anxiety seeks care predominantly through their primary care physician. | |
| Care Model
The patient is receives care in a medical practice that participates in a Collaborative Care Model (CoCM) where behavioral health services are integrated into the primary care setting. They receive Cognitive Behavioral Therapy (CBT) and a prescription for a selective serotonin reuptake inhibitor (SSRI). |
Limitations
While effective for mild to moderate anxiety or depression, collaborative care models often lack the intensity or specialty training needed to manage complex behavioral symptoms tied to serious illness. Time-limited therapy and medication management may not address existential distress, trauma, or grief. Primary care teams may also lack capacity to coordinate with palliative care and CoCM does not focus on such collaborations. |
| A patient with schizophrenia and co-occurring alcohol use disorder is diagnosed with advanced liver disease. | |
| Care Model
The patient receives services through an Integrated Dual Diagnosis Treatment (IDDT) team, including case management, peer support, and psychiatric medications.
|
Limitations
SPMI-focused models like IDDT often operate in behavioral health silos and may not integrate well with specialty medical providers. As a result, coordination with hepatology or palliative care teams may be limited, leading to gaps in treatment planning, poor symptom control, and misalignment with the patient’s goals of care. Providers may struggle to navigate informed consent or advance care planning. If the patient does not have the proper insurance, there is no sustainable payment mechanism for these services. |
| An elderly woman with moderate-stage Alzheimer’s experiences increasing agitation and behavioral disturbances. | |
| Care Model
She is enrolled in the Care Ecosystem model, intended for dementia care, which provides caregiver support and structured behavioral interventions, and is prescribed low-dose Quetiapine.
|
Limitations
While the model helps reduce caregiver stress and behavioral crises, it may not include direct medical management or in-home services to address progression of illness. Access to specialists such as geriatric psychiatrists or neurologists will continue to be challenging. The reliance on caregiver capacity also assumes a level of support not all families can provide, contributing to early institutionalization. Finally, current reimbursements models do not provide sufficient support for program like Care Ecosystem, limiting access. |
Policy Priority Areas
The policy areas below mirror those advanced by the Center for Behavioral Health and reflect unique considerations for people with serious illness. Specifically, CTAC recommends the following:
Payment
- Expand Medicare and Medicaid coverage for integrated behavioral health services across serious illness settings, including caregiver training and in kind support, behavioral health consultation in specialty care, and non-pharmacologic dementia interventions.
- Develop bundled payments and population-based models that support comprehensive, interdisciplinary teams across both primary and specialty care.
- Fully enforce the Mental Health Parity and Addiction Equity Act to ensure behavioral health coverage parity in serious illness care.
Quality Outcomes
- Develop and adopt quality measures that reflect the behavioral health needs of people with serious illness, including patient-reported outcomes, caregiver well-being, and functional and cognitive status.
- Incorporate behavioral health metrics into serious illness payment and delivery models (e.g., ACOs, hospice, palliative care) to drive integrated care.
Workforce
- Expand loan repayment programs and training incentives for behavioral health professionals trained in geriatrics or serious illness.
- Support interdisciplinary geriatric psychiatry and palliative care training for physicians, nurses, social workers, and peer supporters.
- Develop and fund mobile behavioral health units and consultation teams embedded in serious illness and dementia care networks.
- Remove CMS restrictions preventing social workers from billing for advance care planning.
Data Infrastructure
- Require Medicaid and Medicare programs to report quality and utilization metrics stratified by behavioral health condition and serious illness to identify disparities and target improvements.
- Support development of decision support tools that are adaptable to cognitive decline and behavioral health complexity and enable data inputs (with appropriate consent) from all relevant providers.
Access to Evidence-Based Care
- Fund studies focused on older adults and individuals with co-occurring serious illness and behavioral health conditions, including those with SPMI and substance use disorders.
- Promote research into hybrid care models that integrate behavioral health into specialty settings (e.g., oncology, hepatology, geriatrics).
- Continue to experiment with direct-to-caregiver supports, such as in-home aide support, case managers, or even direct payments, to alleviate burden and assist in moments of crisis.
- Promote use of psychiatric advance directives (PADs) for individuals with SPMI.
- Support legislation like the Uniform Health-Care Decisions Act (UHCDA) and H.R. 1867 to modernize consent and expand telehealth.


