
 C-TAC has long advocated for integrating community-based services to meet the health-related social needs of those with serious illness. Lately, efforts at both the federal/Medicare and state/Medicaid level will provide meaningful services to address these needs:
C-TAC has long advocated for integrating community-based services to meet the health-related social needs of those with serious illness. Lately, efforts at both the federal/Medicare and state/Medicaid level will provide meaningful services to address these needs:
- New Medicare billing codes – As C-TAC noted before, CMS now has new payment billing codes for key components of a comprehensive assessment and to better meet peoples’ social needs. These codes and other new ones will help address those needs and link to resources to meet them:
- Caregiver Training Services – pays providers to provide education to family caregivers to help their loved one better manage their illness.
- Principal Illness Navigation – pays for certified navigators for those with serious illness that incorporates their goals and values.
- Community Health Integration – pays for the time to make referrals to community services.
- Social Determinants of Health (SDOH) Risk Assessments – pays for providers doing the increasingly required SDOH assessments.
- Community Health Workers (CHW)/Peer Supports – pays for these important community resources.
- Street Medicine – As of last October (2023), CMS began allowing public and private insurers to pay “street medicine” providers for medical services they deliver anyplace homeless people might be staying.
- Behavioral Health Expansion – pays family and marriage therapists for their care for Medicare patients and expands access in other ways as well.
- Medicaid 1115 Waivers – These waivers let states customize their Medicaid programs and some now allow for new services to address:
- Serious persistent mental illness (SPMI) & substance use disorder (SUD)
- High-needs high-cost/high utilizers
- Chronic, co-morbid, and complex conditions
- Disabilities, long-term services and supports (LTSS)
- Transitioning from institutional settings to the community
- Homelessness
- Child welfare or justice system involvement
- Food security/medically tailored meals
- Transportation support
- Other state options – States can also address SDOH/HRSN through a variety of other options such as
- Home and Community-based services through state plans amendments and 1905(a), 1915(i) and (c) waivers. These can provide housing supports, employment supports, peer services to facilitate staying at home, and health homes and case management.
- CMS Innovation Center’s Accountable Health Communities model
As a result, five states now cover HSRNs through their state programs: Arkansas, Arizona, California, and Massachusetts.
- California specifically has an unprecedented 5-year, multi-billion-dollar plan, CalAIM, to:
- Advance the Medi-Cal (Medicaid) program
- Make it more streamlined and community-based
- Expand the network of community partners
- Ensure Medi-Cal services are more equitable, coordinated, and person-centered
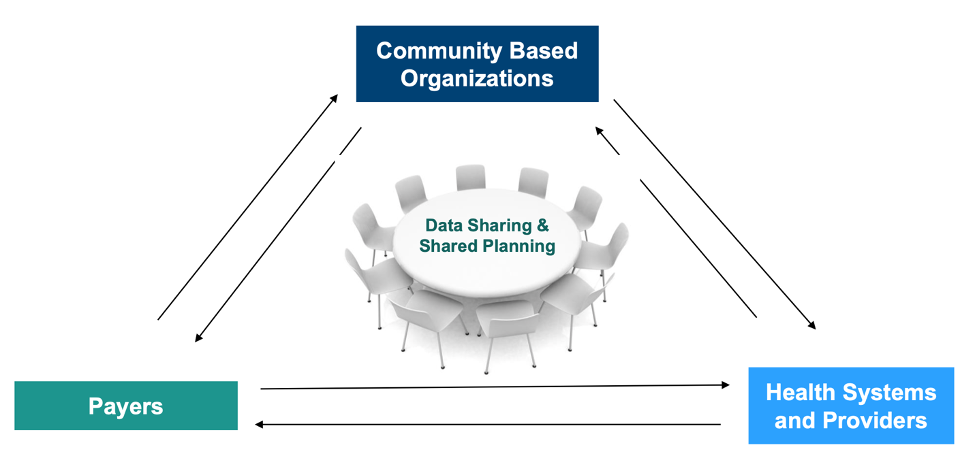
Here is a visual model of how all the elements are working together.
Our thanks to partner Lauran Hardin, MSN, CNL, FNAP, FAAN, an expert in this area, who is advising CMMI and several states in these efforts and provided information for this post.


